HEART FAILURE 2
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and diagnosis with a treatment plan.
You can find the entire real patient clinical problem in the following link:
https://himabindu5.blogspot.com/2020/05/hello-everyone.html
Following is my analysis of the patient's problem. The problems in the order of priority I found are:
You can find the entire real patient clinical problem in the following link:
https://himabindu5.blogspot.com/2020/05/hello-everyone.html
Following is my analysis of the patient's problem. The problems in the order of priority I found are:
- Chest pain since 2 months
- Palpitation since 2 months
- Dyspnea since 2 months
- Pedal edema since 1 week
CHEST PAIN
Patient presented with chest pain since 2 months,on the left side more on the epigastrium and was non radiating and associated with palpitations.Palpitation are gradual in onset.Is it VOLUME OVERLOAD??
- no history of increase in pain during inspiration
- no history of increase in pain while lying in supine.
- no history of increase in pain after taking food
- no history of increase in pain during movement
From the above history I think it is related to HEART.
SHORTNESS OF BREATH (DYSPNEA)
Patient presented with shortness of breath, which is progressive and NYHA class 3-4.
Some of the structures (differential) related to dyspnea are:
- Cardiac
- Respiratory
- Anemia
- Renal
- Metabolic
- Neuromuscular
- Drugs
- No history of cough ,cold ,hemoptysis. This excludes respiratory cause of dyspnea
- No history of facial puffiness.There is history of oliguria since 1 week.Is there any renal pathology??
- No history of chronic use of drugs such as NSAIDs, steroids.
- No history of muscle pain,muscle loss, tingling and numbness.This excludes neuromuscular involvement.
- Not a known case of diabetes mellitus
- History of PND since 2 months which is progressive and increased since 10days.
PEDAL EDEMA
Patient presented with progressive bilateral pitting type of pedal edema upto ankle.
Differential diagnosis for pitting type of pedal edema are:
- Heart failure
- Kidney failure
- Liver failure
- No history of periorbital edema,no burning micturation. There is history of oliguria .
- There is no history of ascites..so there might not be hepatic pathology.
From the above details I think there is cardiac pathology.
After analyzing the above complaints , I am opinion that it is HEART FAILURE. Most of the features are suggestive of LEFT HEART FAILURE.What is the reason behind left ventricular failure????
LEFT VENTRICULAR FAILURE
Looking in examination findings:
- apex beat is felt at downward and outward in the 6th intercostal space in anterior axillary line,suggestive of CARDIOMEGALY.
- loud S1 is heard, which can be seen in MITRAL STENOSIS ,TACHYCARDIA, HYPERKINETIC STATES,SHORT P-R INTERVAL.
- splitting of S2 with loud P2 component, suggestive pulmonary hypertension.
- elevated JVP - prominent a wave.
Investigation
- Chest X-RAY - cardiomegaly is conformed
 |
- 2D ECHO- calcified mitral valve
- ECG-
 |
- LFT- raised levels of bilirubin ,SGOT and ALP ,which maybe suggestive of liver failure due to heart failure.
 |
- RFT- creatinine level are normal.Urea level are elevated which can be seen in heart failure.SO there is no renal failure .
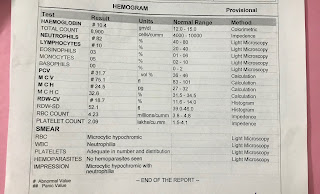
- Hemogram-suggestive of microcytic hypochromic anemia.Is it due to any Chronic infection???
 |
 |
From the above finding I am of the opinion that MITRAL STENOSIS has lead to heart failure.
What might be the cause of mitral stenosis.Some of the causes are:
- Rheumatic fever
- Infective endocarditis
- Severe mitral annular calcification
Treatment that is given:
- INJ.LASIX 2amp in 50ml NS
- nebulization with budecort 12th hourly
- inj.amiodarone 300mg (2amp) at 6ml/hr
- T. ecosprin 75mg/PO/OD
- inj.pantop 40mg/OD/iv
- fluid and salt restriction
Treatment that can be given if not responding to drugs:
- Percutaneous balloon mitral valvulotomy
- Mitral valve surgery
SOME OF THE QUESTION THAT SHOULD BE ANSWERED ARE:
- IS THERE PULMONARY HYPERTENSION????
- IS MICROCYTIC HYPOCHROMIC ANEMIA DUE TO CHRONIC INFECTION???
- WHAT MAY BE THE CAUSE OF ABSENT P WAVE (AS NORMALLY IN MITRAL STENOSIS P MITRALE SHOULD BE SEEN)
- WHAT COULD BE THE REASON BEHIND VOLUME OVERLOAD WHICH CAUSED PALPITATIONS.

[29/05/20, 6:19:50 PM] MBBS 2016 student: Sir ,In this case patient has oliguria ,Dyspnea and pedal Edema .These features are present in renal failure also. How can we eliminate it
ReplyDeletehttps://himabindu5.blogspot.com/2020/05/hello-everyone.html
[29/05/20, 10:04:59 PM] Post residency PG 1: Look up Cardio renal syndromes and let me know which type will it fit into
[29/05/20, 10:05:50 PM] MBBS 2016 student: But Now I found that creatine was normal in this case
[29/05/20, 10:06:03 PM] MBBS 2016 student: I don’t think there is some renal cause
[29/05/20, 10:06:41 PM] MBBS 2016 student: Only urea is elevated which can be seen in heart failure
[29/05/20, 10:06:57 PM] MBBS 2016 student : But what might caused oliguria??
[29/05/20, 11:14:46 PM] MBBS 2016 student: I think it is type 2 chronic CRS
ReplyDelete[29/05/20, 8:52:00 PM] MBBS 2016 student: He has oliguria Dyspnea pedal edema . These features are also suggestive of renal pathology
[29/05/20, 8:52:27 PM] MBBS 2016 student: And wheeze is present in respiratory conditions
[29/05/20, 8:52:54 PM] MBBS 2016 student: How can this be eliminated and only cardiac cause is diagnosed by history
[29/05/20, 8:57:06 PM] MBBS 2016 student: Why is ALP elevated
[29/05/20, 10:28:49 PM] Intern 2015 1: Yes that’s true and for that we got an rft done which is pretty much fine to rule out renal pathology
[29/05/20, 10:29:08 PM] Intern 2015 1:Umm that’s because she has cardiac failure
[29/05/20, 10:29:42 PM] MBBS 2016 student: ALP is related to liver and bone?
[29/05/20, 10:31:12 PM] Intern 2015 1: She has MS that’s causing her left heart failure (presenting with pnd and all..) and that’s causing rhf, affecting her liver.. so that’s what is making the enzymes elevated
[29/05/20, 10:32:14 PM] MBBS 2016 student: I was thinking ALP is not that much specific to the heart
[29/05/20, 10:34:00 PM] Intern 2015 1: Nope I don’t think so
[29/05/20, 10:34:11 PM] MBBS 2016 student : Ok