CASE DISCUSSION
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and diagnosis with a treatment plan.
You can find the entire real patient clinical problem in the following link:
http://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html#comment-form
Following is my analysis of the patient's problem. The problems in the order of priority I found are:
You can find the entire real patient clinical problem in the following link:
http://classworkdecjan.blogspot.com/2019/05/42-f-with-severe-regular-edema-with_17.html#comment-form
Following is my analysis of the patient's problem. The problems in the order of priority I found are:
- Swelling(edema)
- Severe headache
- Muscle weakness
- Mouth ulcers
- Sensory processing disorder
- Excessive hair growth
Swelling
Swelling is present since 1 year age. It is mostly present on face and abdomen. Swelling aggravated on exposure to smoke, emotional stress,physical activity, certain drugs such as sulfa drugs, anti-malarials, and by taking foods such as fava beans. Swelling was associated with fatigue, breathing problems and tachycardia.
She also presented with severe jaundice at the time of birth.Urine is reduced(oliguria) and yellow in color.
She also had hemolytic episodes after a history of travelling.
Differential Diagnosis for swelling
- Cardiac failure
- Kidney problems
- Chronic severe anemia
Diagnosis
This above mentioned complaints are the features seen in increased oxidative stress. It is seen in a genetic disorder - G6PD deficiency.
- She developed hemolytic episodes(swelling) after exposure to the triggering factors.
- Jaundice at birth can be explained by hemolysis
- Excessive destruction of RBC can also damage kidney.This explains oliguria in the patient.
- Due to decreased levels of hemoglobin, oxygen to the tissues also reduced leading to breathing difficulties
- Due to oxidative stress ,there may be amyloid plaques in brain which explains loss of memory.
G6PD Deficiency
Pathophysiology
Normally due to metabolic processes free radicals are released. To neutralize these free radicals, body produces anti-oxidants such as glutathione. This glutathione in reduced state donate electrons to the free radical and gets converted into oxidized glutathione.
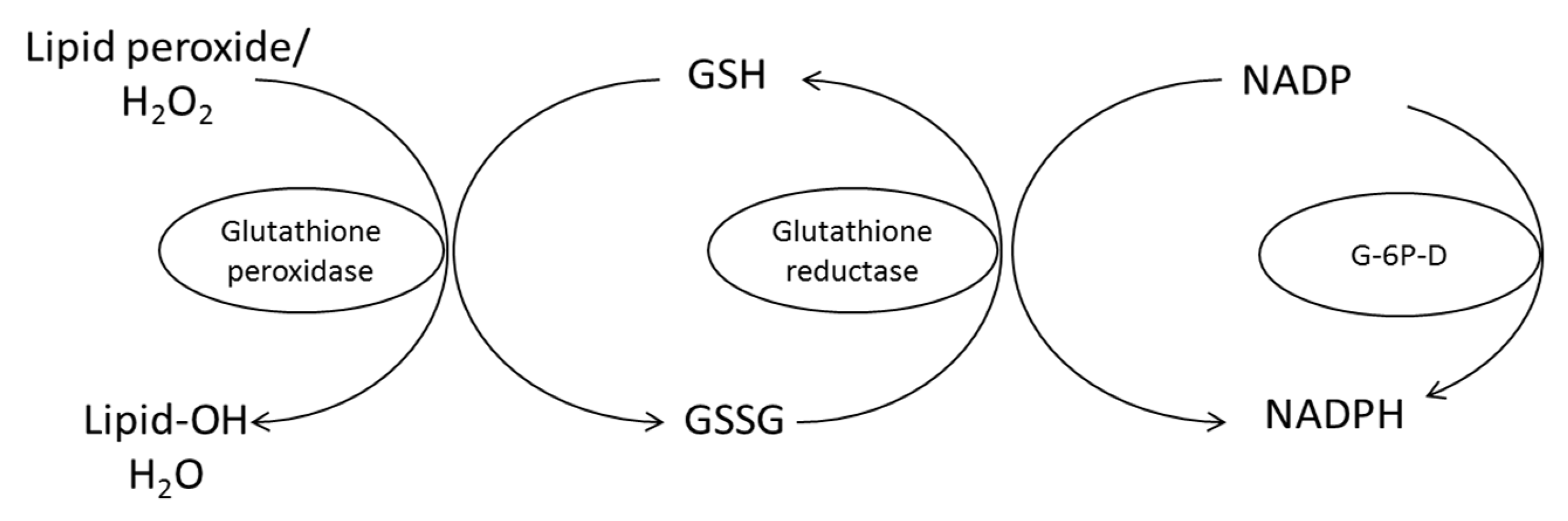
The oxidized glutathione in the presence of glutathione reductase gets converted into reduced glutathione by converting NADPH to NADP. To replenish the NADPH, G6PD is used. G6PD reduces NADP to NADPH by oxidizing G6P(metabolite of glucose).
In case of G6PD deficiency which is X-linked recessive disorder,
Decreased levels of G6PD
↓
Decreased NADPH
↓
Decreased production of reduced glutathione
Due to the absence of glutathione, there is increase in free radicals leading to oxidative stress. Free radical causes hemolysis and hemoglobin molecules are damaged. Damaged hemoglobin precipitates in RBC leading to the formation of heinz bodies. Macrophages recognize the heinz bodies and engulf them, leading to the formation of bite cells. Often, only old RBCs are at risk of lysis. Therefore, hemolytic episodes are limited when young RBCs are formed.
Triggering factor in this case
- foods-fava beans
- drugs-antimalarials
- infections- pt also had a history of pneumonia.Chronic infection triggers immune cells to to fight against the organism.This leads to release of free radicals which damage healthy cells and cause inflammation.In case of oxidative stress (which pt as due to G6PD deficiency),it triggers te inflammatory response more and releases more free radicals and cycle repeats which worsens the symptoms.
- smoke
- exertion
Investigations
Complete blood picture:
- decrease in hemoglobin
- increase in reticulocytes(to compensate the loss of RBC)
- increase in LDH
- increase in bilirubin
- decrease in haptoglobulin
Peripheral smear:
- bite cells
- heinz bodies
Enzyme detection - G6PD level should be detected
Genetic test-she underwent genetic testing at the age of 33yrs and was conformed by G6PD deficiency.
Treatment
- She has taken ribose for swelling
- Avoid exposure to triggering factors
- She is taking serine which helped her in treatment of oliguria.
others
- Salt restriction
- Blood transfusions
- antioxidant vitamins
Severe Headache
She has severe headache since 2 years of age. Headache is sudden in onset and very severe. She develops aura before developing headache.
Aura - she develops rainbow colors, temporary blindness
left hand numbness
falling to left side (ataxia)
stuttering of speech
vertigo
Severe headache was aggravated with menses, excess stress and use of birth-control pills.
At the age of 34 years she had one episode of headache on the left side and was associated with nasal discharge for ten minutes.
Diagnosis
In the above mentioned complaints, patient may be suffering from hemiplegic migraine.
Hemiplegic Migraine
Mutations in genes can lead to break down of body's ability to make certain proteins without which nerves cells have trouble in sending or receiving signals(serotonin).
Triggering factors in this case
- Intense physical activity
- Skipping of meals
- Travelling
- Exposure to smoke
- Stress
- Use of birth control pills
- Decreased sleep
Investigations
- CT and MRI
- Tests of heart and blood vessels to rule out blood clots
Treatment
She has taken triptans for migraine.
Other medications that can be used are CGRP inhibitors.
Muscle Weakness
She develops muscle weakness fatigue on exertion.
Differential Diagnosis
- AMPD-1 deficiency
- Anemia
AMPD-1 Deficiency
It is inherited autosomal recessive disorder caused due to mutations in AMPD-1 gene. This gene makes enzyme AMP deaminase which plays a role in producing energy in skeletal muscles. Mutations in this gene disturbs the function of AMP deaminase leading to muscle problems.
Investigations
Genetic test: She was diagnosed for AMPD-1 deficiency heterzygous.
Treatment
She has been taking ribose - 2grams every hour in water.
Other medications which can be used are citrate monohydrate.
Mouth Ulcers
She develops mouth and vaginal ulcers when exposed to stress.These were more often until she took pnemonia vacccine at the age of 28 years.She also has blurring of vision ang head ache.She also has a history of longterm knee and hip pain.She also had butterfly rash on the face.
Differential Diagnosis
- SLE
- Behcet's disease
Behcet's Disease
It is a rare disorder that causes blood vessel inflammation throughout the body.It is often associated with many mutation.It presents as mouth ulcers,eye problems,skin rashes and joint pains.
Investigations
- Mouth sores which has recurred 3 times in 12 months.
- Blood tests
- Pathergy test
- Tests to rule out SLE.
- Genetic testing
Treatment
- Colchicine
- Corticosteroids
- Medications that supress immune system
Sensory processing disorder
- higher pain tolerance
- uncomfortable with physical contact
- feels angry
- used to throw tantrums
These features are suggestive of sensory process disorder.
Excessive hair growth
She has excessive hair growth on face, neck, toes and legs since childhood.
She has chronic abdominal pain at the time of menses.
Differential Diagnosis
- Congenital adrenal hyperplasia
- PCOS
Investigations
- Cortisol level -elevated
- CT scan - showed multiple ovarian cysts.
Treatment
- Spironolactone
- Eflornithine
- Anti androgens
- electrolysis
References - Various internet sources
Avinash Sir's case
ReplyDeleteWhat is the efficacy of the various interventions she has been using and what is the sensitivity and specificity of the various diagnostic interventions she has undergone?
What other history, clinical findings and investigations would you need to solve her problem.
[5/16, 8:19 PM] +91: Other things that can be asked are
ReplyDelete1)Nattokinase can worsen bleeding disorders.Will that not affect her as she has VWF mutations
2)why is she consuming salt?Does that not lead to more swelling
3)She has history of rashes and joint pain.So she should be also suspected for SLE and RA.She should be investigated for that.
4)she has been prescribed by colchicine this can have effect on muscle (muscle damage)
[5/16, 8:24 PM] +91: Alternatively for colchicine for treatment of Behcet corticosteroids can also be used
[5/16, 8:24 PM] +91 : Or any medications that can suppress immune response
[5/16, 8:28 PM] Rakesh Biswas: 1) Why is she on nattokinase? How was it supposed to be helping her even if it may not harm her (although you are suggesting it might harm too)?
2) Good question. Why do some people crave salt? What are the underlying metabolic mechanisms?
3) What are the most important clinical and or lab data to diagnose SLE or RA? Are these mentioned in the data provided in her online record?
4) What is the most important clinical and or lab data that can make us diagnose Behchets? What can this diagnosis do to help solve her multiple issues?
5) What was the cochicine prescribed for?
[5/16, 8:28 PM] Rakesh Biswas: What are her current symptoms of significantly increased immune activity?
[5/16, 8:28 PM] Rakesh Biswas: 1) Why is she on nattokinase? How was it supposed to be helping her even if it may not harm her (although you are suggesting it might harm too)?
ReplyDelete2) Good question. Why do some people crave salt? What are the underlying metabolic mechanisms?
3) What are the most important clinical and or lab data to diagnose SLE or RA? Are these mentioned in the data provided in her online record?
4) What is the most important clinical and or lab data that can make us diagnose Behchets? What can this diagnosis do to help solve her multiple issues?
5) What was the cochicine prescribed for?
[5/16, 9:21 PM] Sai Bhavana 2015 Kims: There are no specific tests for diagnosis of behcets disease.Diagnosis is mostly based on signs and symptoms sir
mouth ulcer at least 3 times in 1year with one of the following signs
Genital sores
Eye problems
Skin rashes
Behcets leads to inflammation of blood vessels which can cause swelling in arms and legs
This might be one of the reason for her swelling.
[5/16, 9:23 PM] Sai Bhavana 2015 Kims: Colchicine is prescribed for behcets as it has anti inflammatory mechanisms
[5/16, 9:24 PM] Sai Bhavana 2015 Kims: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4656054/
[5/16, 9:59 PM] Rakesh Biswas: What is the efficacy of cochicine in Behchets? Are their any randomized controlled trials in Behchets to show that it has efficacy in Behchets?
[5/16, 9:59 PM] Rakesh Biswas: What is the efficacy of cochicine in Behchets? Are their any randomized controlled trials in Behchets to show that it has efficacy in Behchets?
ReplyDelete[5/17, 8:54 AM] Sai Bhavana 2015 Kims: https://onlinelibrary.wiley.com/doi/full/10.1002/1529-0131(200111)44:11%3C2686::AID-ART448%3E3.0.CO;2-H
[5/17, 8:57 AM] Sai Bhavana 2015 Kims: There are randomised controlled trails done for Colchine use in Behcet’s disease.These studies showed that use of colchicine can reduce genital ulcers,arthritis especially in women
[5/17, 9:16 AM] Rakesh Biswas: Tell us the results of one RCT in a PICO format.
How many patients were studied?
How many received cochicine?
How many received placebo?
What were the outcomes in each group?
[5/17, 10:14 AM] Sai Bhavana 2015 Kims: Sir total no of pts are 169.They didn’t mention separately those under colchicine and placebo.
ReplyDelete[5/17, 10:15 AM] Rakesh Biswas: Do you have the full text link to the study?
[5/17, 10:15 AM] Sai Bhavana 2015 Kims: Referencing to that link sir
[5/17, 10:15 AM] Sai Bhavana 2015 Kims: I mentioned the link in pdf sir
[5/17, 10:15 AM] Rakesh Biswas: Good.
But then it's apparently wrong if you put 169 in both groups? ��
[5/17, 10:16 AM] Sai Bhavana 2015 Kims: Yes sir I didn’t understand how to put them so
[5/17, 10:16 AM] Sai Bhavana 2015 Kims: I will send the link
[5/17, 10:18 AM] Rakesh Biswas: Yes please. It's not opening from the PDF
[5/17, 10:18 AM] Sai Bhavana 2015 Kims: https://clinicaltrials.gov/ct2/show/NCT00700297
[5/17, 10:21 AM] Rakesh Biswas: This is their trial registry link. You will have to search for their finally published study ��
[5/17, 10:22 AM] Sai Bhavana 2015 Kims: Ok sir
[5/17, 10:28 AM] Sai Bhavana 2015 Kims: https://pubmed.ncbi.nlm.nih.gov/19597921/
[5/17, 10:35 AM] Rakesh Biswas: ��How did they calculate "overall disease activity index, the IBDDAM" and when they say "worsened from 3.17 to 3.63" or "improved from 3.35 to 2.75" how do we visualize the effect size to ascertain if it was clinically significant?
Also when they say, "Oral aphthosis, genital aphthosis, pseudofolliculitis, and erythema nodosum improved significantly with colchicine but not with placebo" how do we make out how much significantly? ��
[5/17, 4:08 PM] Sai Bhavana 2015 Kims: This is another RCT trail conducted on 116 patients.
ReplyDeletehttps://onlinelibrary.wiley.com/doi/full/10.1002/1529-0131%28200111%2944%3A11%3C2686%3A%3AAID-ART448%3E3.0.CO%3B2-H
[5/17, 4:25 PM] Rakesh Biswas: What were the outcomes here?
[5/17, 4:28 PM] Sai Bhavana 2015 Kims: In females
91% were arthritis free with colchicine compared to 64% in placebo
There few new attacks of erythema nodosum and genital ulcer with colchicine compared to placebo
[5/17, 4:29 PM] Sai Bhavana 2015 Kims: Oral ulcers and folliculites did not show significant difference
[5/17, 4:29 PM] Rakesh Biswas: This one is better. Now look at their outcomes.
"At the end of the trial, 91% of the female patients in the colchicine arm remained arthritis free as compared with 64% in the placebo arm"
If we were one of the 64 out of 100 people receiving placebo and remained free of arthritis what would be the problem in just taking placebo?
Now similarly look at the other outcomes
[5/17, 4:30 PM] Rakesh Biswas: Second line: how many?
[5/17, 4:31 PM] Sai Bhavana 2015 Kims: Erythema nodosum
78% - colchine
39% - placebo
[5/17, 4:32 PM] Sai Bhavana 2015 Kims: Genital ulcers
89% - Colchicine
46% -placebo
[5/17, 4:50 PM] Rakesh Biswas: Looks like more people had newer attacks with colchicine than placebo? Contrary to what was shared in that line earlier? ��
What do these numbers mean?
[5/17, 5:17 PM] Sai Bhavana 2015 Kims: 78% pts were free from erythema nodosum when treated with colchicine
[5/17, 5:19 PM] Rakesh Biswas: What was the study duration that they were found to be free? What if it came after the study completion?
[5/17, 5:19 PM] Sai Bhavana 2015 Kims: Yes sir
[5/17, 5:20 PM] Sai Bhavana 2015 Kims: But then how can we know the efficacy correctly sir
[5/17, 5:20 PM] Sai Bhavana 2015 Kims: Every trail has only limited duration
[5/17, 5:22 PM] Sai Bhavana 2015 Kims: If it returns after the completion of the study (treatment) then do pts need to take the treatment for lifelong sir??
[5/17, 5:23 PM] Sai Bhavana 2015 Kims: Duration of study was 2yrs sir
[5/17, 5:24 PM] Rakesh Biswas: Yes isn't that a major limitation on how we do current research? Hope your generation will be able to change it
[5/17, 5:24 PM] Sai Bhavana 2015 Kims: Yes sir we will try to improve it
[5/17, 5:25 PM] Sai Bhavana 2015 Kims: Thank you sir for asking these questions and making me think in different way.I never had a a clarity on this trails now but now because of ur questions I learned a lot today
[5/17, 5:26 PM] Rakesh Biswas: Well two years is a good duration and the affected and unaffected population numbers look clinically significant but then if you try to imagine each of these trial participants even the 46 out of 100 who didn't develop fresh lesions on placebo what difference would the colchicine really have made in their lives?
[5/17, 5:29 PM] Sai Bhavana 2015 Kims: This might be related to one symptom maybe other symptoms might not be affected by the placebo effect
Suppose if a person had results with placebo for erythema nodosum but not for arthritis
[5/17, 5:29 PM] Sai Bhavana 2015 Kims: In the same person
[5/17, 5:33 PM] Rakesh Biswas: Very good thinking. We need to check what happened to each individual. Here the data appeared to be focused on the cochicine and disease data points and the individual trial participants appear to have been stripped off their individuality?
[5/17, 5:44 PM] Sai Bhavana 2015 Kims: Yes sir
ReplyDelete[26/05/20, 2:15:46 PM] MBBS 2016 student: Sir in this case due to increased oxidative stress there in increased hemolysis which could have lead to kidney injury
[26/05/20, 2:16:10 PM] MBBS 2016 student: Kidney injury has lead to edema
[26/05/20, 2:18:23 PM] MBBS 2016 student: Other mechanisms for edema are
Increased hydrostatic pressure
Decreased plasma oncotic pressure
[26/05/20, 4:30:49 PM] Post residency pg 1: So how is she surviving with her kidney injury for how many years? What is the way to confirm her kidney injury? What is her creatinine?
[26/05/20, 4:31:44 PM]Post residency pg 1:These are the only important mechanisms.
Do you know of any other mechanism?
[26/05/20, 4:32:15 PM] MBBS 2016 student: Yes sir
Other mechanisms are
Lymphatic obstruction
Salt and water retention
[26/05/20, 4:36:14 PM] MBBS 2016 student: Increased permeability can also cause
[26/05/20, 4:47:51 PM] MBBS 2016 student: Diagnosis can be made on creatinine levels ,urine output.but for this patient creatinine is normal
[26/05/20, 4:49:57 PM] Post residency pg 1: So she didn't have any evidence of renal injury isn't it?
[26/05/20, 4:50:37 PM] MBBS 2016 student: Yes sir
[26/05/20, 4:51:53 PM] MBBS 2016 student: Sir the why does she develop Edema only when exposed to triggering factors for oxidative stress
[26/05/20, 4:52:41 PM] Post residency pg 1: What are the triggering factors and how can you be sure there is a correlation or causation?
[26/05/20, 4:53:59 PM] MBBS 2016 student: Triggering factor for were
Fava beans
Antimalarials
Exposure to smoke
Exertion
[26/05/20, 4:54:33 PM]MBBS 2016 student:And in history she mentioned that she used swell up after exposure to this factors
[26/05/20, 4:55:11 PM] MBBS 2016 student: So I assumed that there may be some relation with oxidative stress
[26/05/20, 7:47:05 PM] Post residency pg 1: Good 👍
[28/05/20, 11:26:11 AM] MBBS 2016 student: While going through this case again,I think that edema in this case could be due to chronic anemia
Chronic anemia leads to reduced peripheral vascular resistance which leads to activation of RAAS mechanism leading to salt and water retention
And low Hb conc can lead to reduced inhibition of NO which leads to vasodilation and again activated raas mechanisms leading to edema
[28/05/20, 11:31:12 AM] Post residency pg 1: What was is her Hb?
Check out the current updates of this patient in the original blog posted by our global student
[28/05/20, 11:34:21 AM] MBBS 2016 student: Hb was normal sir but she has G6PD deficiency which leads to hemolysis
[28/05/20, 11:34:33 AM] MBBS 2016 student: How can her Hb be normal sir
[28/05/20, 11:34:52 AM] Post residency pg 1: How many times in her life has she had the hemolysis?
[28/05/20, 11:38:05 AM] MBBS 2016 student: Everytime when she is exposed to triggering factor there must be more oxidative stress and which might lead to hemolysis
[28/05/20, 11:38:22 AM] MBBS 2016 student: And edema
[28/05/20, 11:43:36 AM] Post residency pg 1: Yes how frequent was that and when was her last Hemolytic episode? Ask the original poster
[29/05/20, 8:54:28 AM] MBBS 2016 student: Sir frequency varies depending on triggers, nowadays she has less and last time was 45 days back